VExUS in Nephrology: Case Examples
VExUS is an emerging field, and consequently, its practical application in day-to-day clinical practice is not widely acknowledged. Presented below are selected cases we have published (as of November 2023), each conveying a unique teaching point. Links to the full articles are provided; click on the word ‘case’.
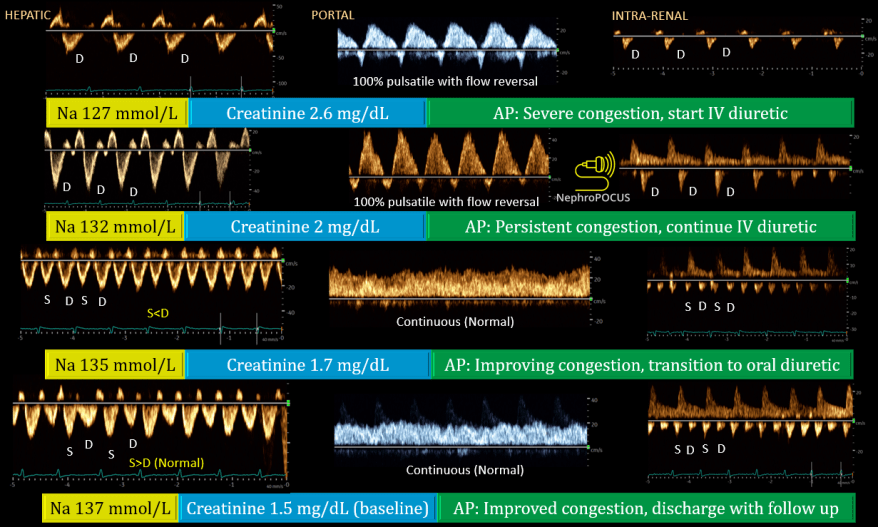
Case 1: This is a classic example showcasing how diuretic therapy led to the simultaneous improvement of all three waveforms (hepatic, portal, and intrarenal) alongside improvement in serum creatinine and sodium levels. It also underscores the general observation that improvement in the portal vein typically precedes that of the hepatic and renal veins. Additionally, it highlights that recovery of the intrarenal venous waveform may be delayed (likely due to renal interstitial edema).
Case 2: This example underscores the dynamic nature of the portal vein waveform. Observe the transition from a pulsatile pattern to a continuous one during fluid removal (in this case, ultrafiltration), and its reversal to a pulsatile pattern with positive fluid balance. This feature renders it an excellent non-invasive monitoring tool at the bedside for patients with tenuous hemodynamic status.

Case 3: This is from the same article that illustrates how we use VExUS in the outpatient clinic. Note how the severity of congestion improved from the initial visit to 3-month follow up with diuretic therapy.

Case 4: This presents a scenario involving a chronically mechanically ventilated patient, where there was progressive improvement observed in hepatic and portal waveforms with ultrafiltration. Additionally, take note of the reversal of the D-sign (interventricular septal flattening) on the parasternal short axis with fluid removal. It also highlights the observation that the inferior vena cava may be chronically dilated in such patients (= shouldn’t be used as a sole POCUS parameter). We used a handheld device to obtain these waveforms and hence no simultaneous EKG.


Case 5: While it is true that hepatic and portal vein waveforms may be abnormal at baseline in cirrhosis, this does not render them useless, particularly if previous imaging indicates near-normal waveforms. This is a case of fluid overload in a patient with biopsy-proven cirrhosis, showcasing improvement in cardiac ultrasound parameters (inferior vena cava size, D-sign) as well as VExUS with fluid removal. Note that the final hepatic waveform appears blunted (with less defined S and D), which is typical in cirrhosis and fatty liver.



Case 6: A case of heart failure where the initial impression (before POCUS) was overdiuresis. However, VExUS demonstrated severe congestion that eventually improved with fluid removal.



Case 7: Another instance where pre-POCUS impression in a patient with worsening serum creatinine and hyponatremia was volume depletion/overdiuresis. POCUS showed the opposite leading to change in management and improvement in waveforms with diuretic therapy. This patient had a dilated IVC at baseline rendering it less useful for monitoring response to therapy.


Case 8: This presents a scenario involving a patient with end-stage renal disease undergoing hemodialysis, with a history of chronic pulmonary hypertension and severe tricuspid regurgitation. In this context, the IVC is anticipated to be chronically dilated, and hepatic vein Doppler often shows S-reversal, making the diagnosis of superimposed fluid overload challenging. However, portal vein Doppler can be valuable in such situations. With an approximate ultrafiltration of 4 liters, observe how the portal vein waveform normalized while the IVC remained persistently dilated.


Case 9: A nice example that underscores the need to avoid excessive reliance on recent imaging or physical examination findings with low sensitivity, such as pedal edema or lung crackles, to guide therapy in heart failure patients. It is now well established that the diagnostic accuracy of POCUS surpasses that of conventional physical examination. Also, don’t forget, hemodynamics are dynamic!

That’s all for now. VExUS is not limited to a specific specialty or clinical setting but falls within the purview of POCUS-competent physicians taking care of patients with changing hemodynamic profiles. Remember to use simultaneous EKG where possible (for precise interpretation of hepatic vein and cardiac Doppler) and interpret VExUS findings in conjunction with cardiopulmonary POCUS and the relevant clinical context. Below is the VExUS grading card if you need a refresher. Happy scanning!

3 Comments »